Download App
Download App

 Doctors for Colon Cancer
Doctors for Colon Cancer  OTC Medicines for Colon Cancer
OTC Medicines for Colon Cancer

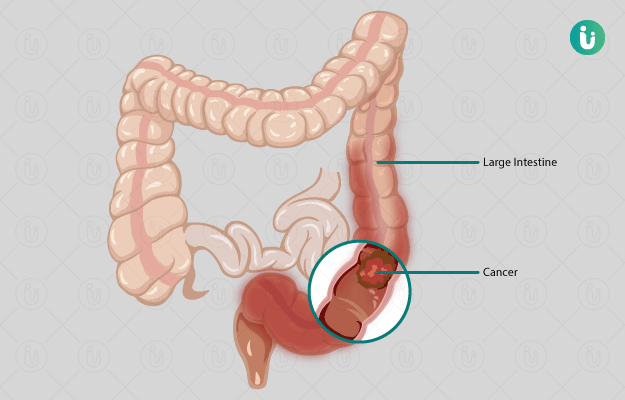
Cancer arising in the colon, also called the large intestine, of the digestive tract, is called colon cancer. It is part of a larger group of cancers affecting the bowel called colorectal cancer, which mainly comprises colon cancer and rectal cancer.
The digestive tract, or the gut, starts at the mouth, through which food passes into the food pipe (or the oesophagus) and then to the stomach, where some of it is digested. The contents of the partially digested food are then passed into the small intestine for further digestion and break down with the help of some other associated glands and organs. After all the food is digested, it is passed from the small intestine to the large intestine or the colon. The colon consists of four segments – the ascending colon, the transverse colon, the sigmoid colon and the descending colon. Here, water and other substances are absorbed and the final waste product is removed from the bowel through the rectum (terminal portion of the large intestine) and anus.