Normally, fluids make up about 60% of the total body weight in men (about 42 litres in a man who weighs 70 kilograms) and about 52% of total body weight in women (about 28.6 litres in a woman who weighs 55 kilograms).
These fluids consist of water and electrolytes like sodium, potassium and chloride. Water alone makes up about 50% to 70% of total body weight in adults. This water could be present inside (intracellular) or outside (extracellular) body cells and helps in transporting nutrients and minerals in the body. The extracellular water could be present inside vessels (both blood and lymph) or in interstitial spaces (spaces around cells). Sodium and chloride are mostly present outside cells, while potassium is mostly present inside cells.
In a body with 42 litres of fluid:
- About 28 litres is present as intracellular fluid (40% of body weight)
- About 14 litres as extracellular fluid (20% of body weight). In extracellular fluid:
- 11 litres (or 15% of body weight in a 70 kg man) is present as interstitial fluid
- 4 litres (about 5% of body weight) is present as plasma (in the blood)
The volume of blood is about 8% of total body weight (about 5.6 litres in a 70kg man).
Maintainance of fluid-electrolyte balance:
Fluid and electrolytes are constantly kept in balance through various processes in the body. You gain fluid through water intake or intake of food and drinks in general. The excess fluid is removed through secretions, including sweat, urine and faeces. A balance between this intake and expulsion of fluids and electrolytes is important to maintain all the metabolic processes in the body.
Also, a balance is maintained between the intracellular and extracellular fluids by the transfer of water in and out of the cell membrane. Water flows to the area where there is a lack of fluids. So if there is less water outside the body cells, it will move from inside to outside and vice versa. However, the process is not so simple: the water must go from the GI tract to the blood before it can reach the body cells.
Read more: How much water to drink in a day
However, both water intake and release from the body can be sensible (obtained from oral fluids and food and released through urine and faeces and sweat) and insensible (gained through metabolic processes in the body and lost through the lungs and skin). Here is a table explaining the total sensible and insensible water intake and expulsion in a man weighing 70 kg:
| |
Route |
Volume: daily average in millilitres (mL) |
| Water gain (sensible) |
Oral fluids
Solid fluids
|
800-1500
500-700
|
| Water loss (sensible) |
Urine
Stools
Sweat
|
800-1500
0-250
0 (however, can go up to 4000 mL)
|
| Water gain (insensible) |
Metabolic water |
300 |
| Water loss (insensible) |
Lungs and skin |
600-900 |
A healthy (70Kg) adult needs around 30-35 mL of water per Kg of their body weight per day. The total normal intake would be around 2,500mL/day and total output would be around 1,400-2,300mL/day.
Here is how the water intake is calculated for any weight type:
- For the first 10 Kg: 100mL/Kg of body weight
- For the next 10 Kg: 50mL/Kg of body weight
- For the rest of the weight: 20mL/Kg
Fluid balance could either be negative or positive:
- Positive fluid balance occurs when fluid intake is greater than fluid output.
- Negative fluid balance occurs when fluid intake is less than fluid output.
The required intake of some electrolytes is as follows:
- Sodium: Under 1,500 milligrams per day (mg/day) in adults. Babies under 12 months should not have more than 400 mg/day of sodium. Infants aged 1-3 years can have up to 800 mg/day of sodium.
- Chloride: 9 mg/day per kilo body weight. So, a man weighing 70 kilos would need 63 mg/day of chloride. Children can have up to 45mg/day of chloride.
- Potassium: Adults need between 3,500mg and 4,700mg of this mineral daily. Children under 3 years of age need about 3,000 mg/day of potassium.
- The other electrolytes present in intracellular and extracellular fluids include calcium, magnesium, HCO3, SO42-, and HPO43-. The fluid also has some proteins.
Read more: Electrolyte imbalance symptoms, causes, diagnosis, treatment, prevention
The volume of fluid in the body is maintained through various systems. However, antidiuretic hormone (ADH) majorly controls fluid balance in the body. ADH is released by the hypothalamus, a gland present in the brain in response to changes in the osmolality and blood pressure in the body. Osmolality indicates the concentration of solutions - how thick or flowy they are - measured in terms of the number of solutes (the component dissolved in a solution) present in per kg of the solution.
The Renin-angiotensin system (RAS) also helps maintain the fluid-electrolyte balance in the body. It signals the body in response to blood pressure changes in the kidneys so the body can store or release more water and/or electrolytes as needed.
Read more: What is the role of renin-angiotensin-aldosterone inhibitors in the treatment of COVID-19?
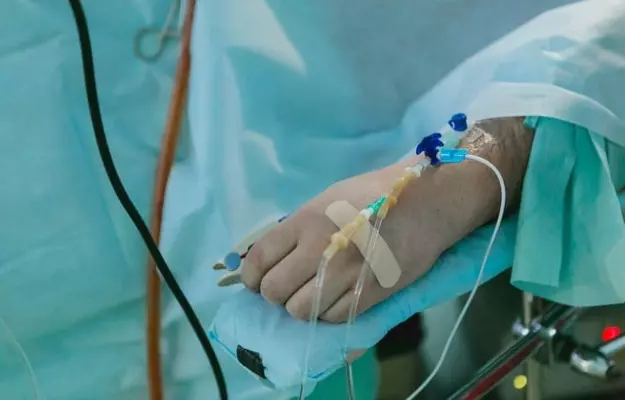
If a person has a severe disease or has an injury, their body will not be able to maintain fluid-electrolyte balance. This is when fluid therapy is needed.



 Download App
Download App