Download App
Download App

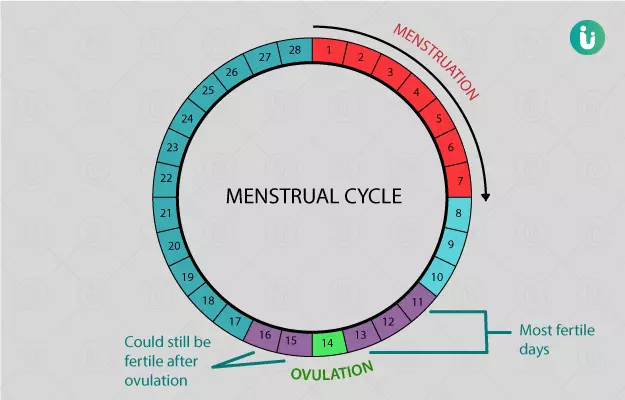




The reproductive life of a female is the stage between the onset of the first menstrual period, or menarche, and the permanent cessation of menses known as menopause. In this phase of a woman’s life, her ovaries produce and release an egg or the female gamete every month; this phenomenon is dubbed ovulation and renders the female capable of becoming pregnant. While the ovaries produce and release the ovum or egg, the uterus prepares itself to host a viable pregnancy, if it should be conceived, by thickening its inner glandular lining (known as the endometrium) and increasing its blood supply. If a pregnancy is not conceived at the end of this cycle, the excess uterine tissue disintegrates and passes out through vaginal bleeding, consisting of blood, mucus and tissue, that typically lasts 2 to 8 days. The menstrual cycle and menstrual period, or menses, are not the same. The entire sequence of events that take place throughout the month in preparation for a possible pregnancy is referred to as the menstrual cycle. The duration of days when a woman experiences bleeding is called the menstrual period, or just period. Menstrual cycles are mediated by the alterations in the levels of reproductive hormones, which bring about different phases of the cycle.
The simultaneous changes taking place in the ovaries and the endometrial layer of the uterus divides the menstrual cycle into two distinct phases – the follicular (ovaries) or proliferative (uterine endometrium) and the luteal (ovaries) or secretory (uterine endometrium). The two phases are separated by the event of ovulation, in which the egg cell is released from the developing follicle in the ovary into the female reproductive tract.
(Read more: Irregular periods)

What is ovulation
Ovulation refers to the phenomenon of the rupture of a fully mature ovarian follicle to release its content – the female gamete called ova or egg. This is a crucial step brought about by the interplay of hormones of the hypothalamus, pituitary and ovaries. The hypothalamus signals the pituitary to signal the ovaries to produce and release the ova. Thus, this hypothalamus-pituitary-ovarian axis is the pillar of the entire process and dysfunction in any of the components will lead to ovulation disorders. Normal ovulation occurs in every menstrual cycle (approximately every month) and is associated with some subtle signs and symptoms in some women. These can even be used to track ovulation, which is particularly helpful to women trying to conceive a pregnancy. Following ovulation, the egg or ova can survive in the female reproductive tract for up to 24 hours; this is called the “fertile window”. Whereas sperm, following sexual intercourse, can remain in the female tract for up to a few days. Therefore, unprotected sexual intercourse in the week leading up to or on the day of ovulation can potentially result in the conception of a pregnancy.
(Read more: Period problems)




















Signs and symptoms of ovulation
While ovulation is a change that occurs in the ovaries, subtle signs and symptoms of the activity can be perceived throughout the body. Some physical signs and symptoms of ovulation are:
- Vaginal discharge or fertile cervical mucus: The discharge is usually more viscous and sticky leading up to ovulation and becomes thinner following it.
- Ovulation pain, mid-cycle pain or mittelschmerz: Discomfort or pain on one side of the lower abdomen and pelvis can arise due to ovulation in some women. It usually arises suddenly and subsides within hours, although it may sometimes last for two or three days. If severe, the pain may be confused with appendicitis and needs imaging studies like an ultrasound. Analgesics can be taken.
- Breast tenderness: Mild analgesics and supportive bras can help assuage breast pain.
- Dip and rise in basal body temperature: The body’s temperature changes throughout the day. The basal body temperature, measured immediately after waking up in the morning, is a good way to compare changes over a period of days. The basal body temperature usually dips before ovulation occurs and remains high for up to two weeks following it.
- Light bleeding or spotting
- Increased sexual drive
Ovulation tracking
Whether to conceive or avoid a pregnancy, ovulation tracking can have useful implications. Home-based options to track ovulation, with varying degree of accuracy, are available to use. Methods to track fertility that employ the expected physical changes of ovulation are called fertility-awareness-based methods. Some examples commonly used by women include, but may not be limited to:
- Calendar method or standard days method: This method is not the most accurate but it is the easiest to employ. The average luteal phase length, which is the period between ovulation and the start of the menstrual period, is considered to be 14 days (for menstruated cycles that last between 21 to 35 days). By charting the length of one’s menstrual cycles for 6 months an average estimate can be drawn of the expected cycle length and the ovulation date can be calculated by subtracting the luteal phase duration (typically 14 days).
- Basal body temperature (BBT) method: Although a tedious task, measuring body temperature with a thermometer and charting it can help detect when ovulation has taken place. Before ovulation, a woman's BBT usually averages between 97°F (36.1°C) and 97.5°F (36.4°C). The body temperature dips a bit just before the ovary releases an egg. Then, 24 hours after the egg's release, body temperature rises to 97.6°F (36.4°C) to 98.6°F (37°C). A sustained rise in basal body temperature (BBT) for three days is taken as a predictor of ovulation having taken place. In order to use the basal body temperature (BBT) method for fertility tracking, morning body temperatures need to be tracked and charted for at least three months.
- Cervical mucus method: Cervical mucus is thick and sticky in the first phase of the menstrual cycle when the uterus is preparing itself to host a pregnancy, to prevent sperm from entering outside the fertility window. As ovulation approaches, the consistency of the mucus thins and it becomes more watery to allow sperm to enter. By charting the consistency of the vaginal discharge daily ovulation can be predicted with reasonable accuracy.
- Symptothermal method: The symptothermal method is considered the most accurate of all fertility-awareness-based methods as it combines basal body temperature (BBT), cervical mucus and calendar methods to predict the fertile window.
- Cervical position method: The position, firmness and openness of the cervix are referred to as its position. Cervical position changes throughout the menstrual cycle. At the start of the cycle, the cervix is firmer, closed and sits lower in the vagina after ovulation, it moves up higher, opens slightly and becomes softer to touch. The method to correctly check cervical position can be learnt from a gynaecologist.
- Ovulation predictor kits: Similar to home urine pregnancy test kits, these kits are strips that detect the presence of the luteinizing hormone (LH) in urine. LH (luteinizing hormone) level surge typically indicates that ovulation will occur within 12 to 36 hours. These tests have to be used for at least 10 days consecutively to increase the accuracy of the result.
- Saliva ferning test kits: Another home-based test kit for ovulation tracking is the saliva ferning test kit, it comes with a viewing scope used to view the deposited saliva. Characteristic fern-like crystals, that resemble the fern plant, are viewed if ovulation has occurred.
(Read more: Pregnancy test)






Ovulation disorders
Broadly speaking, ovulation disorders can be described as two types – oligoovulation (irregular ovulation) or anovulation (absence of ovulation). The reasons for ovulation dysfunction can be related to the hypothalamus, pituitary, ovaries or any other hormonal imbalance. It is important to thoroughly investigate ovulation disorders to treat infertility and improve the overall health of women. Some common ovulation disorders are described below:
- Hypothalamic dysfunction: The hypothalamus is the most important hormone-releasing centre of the body. It regulates the release of all other hormones, including those of the pituitary gland. Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) will not be secreted if the hypothalamus is dysfunctional. Without these two hormones, follicles will not develop in the ovaries, leading to anovulation.
- Hyperprolactinemia: Prolactin is a hormone that is secreted by the pituitary gland. Sometimes, due to pituitary dysfunction or tumours, the circulating levels of prolactin in the blood can be too high. This causes the suppression of estrogen in the ovaries and infertility sets in due to ovulation inhibition.
- Polycystic ovary syndrome: The most common endocrine disorder in young women is also the most common cause of ovulation dysfunction. Polycystic ovary syndrome (PCOS) is linked with obesity, insulin resistance, metabolic syndrome and genetic factors. The patients have irregular, or absent, menstrual periods and ovulation amongst other signs of hyperandrogenism (increased male sex hormone) like acne and hirsutism. On ultrasound, small fluid-filled cysts may be found in the ovaries. Combined oral contraceptive pills are the most common therapy used to regularise the menstrual cycles.
- Primary ovarian insufficiency: Some women may undergo primary or premature ovarian insufficiency when the ovaries stop functioning and producing eggs before the age of 40. This may lead to irregular ovulation, with infrequent ovulatory cycles occurring. This entity is not the same as premature menopause, in which the menstrual cycles stop permanently for 12 months and longer. However, the symptoms of primary ovarian insufficiency may be indistinguishable from premenopausal symptoms.
Find Obstetrician and Gynaecologist in cities
- Obstetrician and Gynaecologist in Bangalore
- Obstetrician and Gynaecologist in Mumbai
- Obstetrician and Gynaecologist in Ghaziabad
- Obstetrician and Gynaecologist in Chennai
- Obstetrician and Gynaecologist in Pune
- Obstetrician and Gynaecologist in Delhi
- Obstetrician and Gynaecologist in Hyderabad
- Obstetrician and Gynaecologist in New Delhi
- Obstetrician and Gynaecologist in Gwalior
- Obstetrician and Gynaecologist in Gurgaon

Doctors for Ovulation
Dr Shernaz Damkevala Dastur
Obstetrics & Gynaecology
25 Years of Experience

Dr. Shravani A
Obstetrics & Gynaecology
3 Years of Experience

Dr Minoo Singh
Obstetrics & Gynaecology
44 Years of Experience

Dr. Godi Anuradha
Obstetrics & Gynaecology
31 Years of Experience
References
- Mihm M, Gangooly S, Muttukrishna S. The normal menstrual cycle in women. Anim Reprod Sci. 2011 Apr;124(3-4):229-36. PMID: 20869180.
- Christin-Maitre S. Physiologie de l'ovulation et mode d'action de la contraception [Physiology of ovulation and mode of action of contraceptive pills]. Rev Prat. 2008 Jan 15;58(1):17-20. French. PMID: 18326357.
- Carlson LJ, Shaw ND. Development of Ovulatory Menstrual Cycles in Adolescent Girls. J Pediatr Adolesc Gynecol. 2019 Jun;32(3):249-253. PMID: 30772499.
- Richard JS. Genetics of ovulation. Semin Reprod Med. 2007 Jul;25(4):235-42. PMID: 17594604.
- Brown J, Farquhar C. Clomiphene and other antioestrogens for ovulation induction in polycystic ovarian syndrome. Cochrane Database Syst Rev. 2016 Dec 15;12(12):CD002249. PMID: 27976369
- Hernández-Angeles C, Castelo-Branco C. Early menopause: A hazard to a woman's health. Indian J Med Res. 2016 Apr;143(4):420-7. PMID: 27377497.