


 Download App
Download App





Summary
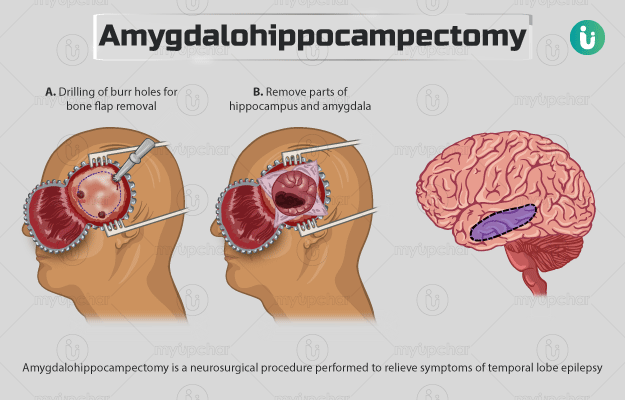
Amygdalohippocampectomy is a neurosurgical procedure performed to relieve symptoms of temporal lobe epilepsy originating in the mesial temporal region. This region consists of five parts, including the hippocampus, amygdala, dentate gyrus, uncus, and parahippocampal gyrus. The temporal lobe of the brain has various functions such as processing memories and producing speech. The symptoms observed in individuals with temporal lobe epilepsy include sensory impairment and repetitive body movements. During the surgery, the surgeon removes some or most parts of the amygdala and hippocampus. You will be given general anaesthesia so that you are asleep during the procedure. After the surgery, you will have to stay in the hospital for about three to four days. The surgery will help improve your quality of life.
- What is amygdalohippocampectomy?
- Why is amygdalohippocampectomy recommended?
- Who can and cannot get amygdalohippocampectomy?
- What preparations are needed before amygdalohippocampectomy?
- How is amygdalohippocampectomy done?
- How to care for yourself after amygdalohippocampectomy?
- What are the possible complications/risks of amygdalohippocampectomy?
- When to follow up with your doctor after an amygdalohippocampectomy?

What is amygdalohippocampectomy?
Amygdalohippocampectomy is a neurosurgical procedure that is done for the treatment of temporal lobe epilepsy.
Epilepsy is a disorder in which abnormal electrical activity in the brain causes a person to have seizures. Seizures result in changes in body movements, behaviour, and level of awareness. When seizures originate in the temporal lobe of the brain, it is called temporal lobe epilepsy. There are two temporal lobes in the body, present on either side of the head by your ears. Many cases of temporal lobe epilepsy originate in the mesial (middle) region of the temporal lobe, which consists of structures like the hippocampus and amygdala. These structures have various functions, including controlling unconscious responses (thirst, hunger, or emotions); processing sounds, smell and memories; producing speech; and interpreting vision. Temporal lobe epilepsy can be caused by various reasons, such as brain injury, inflammation, tumour, infection or alcoholism. Epilepsy most commonly originates from the hippocampus in the mesial temporal lobe, which also affects the amygdala. Therefore, individuals with epilepsy originating from the mesial temporal lobe of the brain respond well to and have better outcomes after amygdalohippocampectomy.
Amygdalohippocampectomy involves the removal of a majority of the hippocampus and some parts of amygdala. Since these regions do not work well in individuals with temporal lobe seizures originating from this region, removal of these parts does not cause disability.

Why is amygdalohippocampectomy recommended?
The surgery is recommended in people with temporal lobe epilepsy originating in the mesial temporal region that does not get resolved by medical treatment. Temporal lobe epilepsy results in seizures wherein your level of consciousness may or may not be impaired. You may experience the following symptoms that may last from a few seconds to two minutes:
- Difficulty speaking
- Deja vu (a feeling of having experienced the current situation before)
- Sensory impairment
- Objects appear smaller or larger than normal
- A sudden sense of anger, fear, joy, or sadness
- Ability to read or understand the spoken word is impaired
- Repetitive movements and behaviours, e.g., excessive blinking, fidgeting, chewing, or lip-smacking
Who can and cannot get amygdalohippocampectomy?
The surgery is not recommended in individuals with the following conditions:
- Severe bilateral hippocampal atrophy with unsupported memory function on the opposite side of the intended surgical side
- Prior surgery for removal of the contralateral temporal lobe or amygdalohippocampectomy
- Extratemporal focal epilepsy (epilepsy originating outside the temporal lobe)
- Idiopathic generalised epilepsy (epilepsy with a genetic basis)
- Temporal lobe epilepsy that may not be localized to the mesial temporal region
- Psychogenic nonepileptic seizures (seizures that do not have a neurological origin)
- Mesial temporal onset seizures with the following features due to a high risk for severe impairment in global memory after the surgery:
- Dominant temporal lobe foci, specifically, individuals with later onset of seizures in adulthood, high preoperative verbal memory, and normal hippocampal volume
- Independent bitemporal onset seizures
What preparations are needed before amygdalohippocampectomy?
Your doctor will order several diagnostic tests before the surgery. Some of these tests include:
- Magnetic resonance imaging (MRI): This test detects tumours and other structural abnormalities in the brain.
- Electroencephalogram (EEG): An EEG test helps measure brain’s electrical activity.
- Positive emission tomography (PET) scan: A PET scan helps identify the origin of the seizure by studying the brain’s metabolism.
- Single photon emission computed tomography (SPECT): This test helps look at the blood flow in the brain and locate the origin of the seizures.
In addition, you will be asked to undergo blood and urine tests to check your overall health. A preoperative assessment will also be conducted wherein the surgeon will take your medical history and ask about any coexisting health condition.
You will be given the following instructions before the surgery:
- Share a list of all the medicines that you take, including herbs and over-the-counter medications.
- Tell the doctor if you are pregnant or have any allergies.
- If you are taking any blood-thinning medicines (warfarin, aspirin, or ibuprofen), the surgeon will ask you to discontinue them about a week before the surgery.
- Remove body piercings, nail polish, and make-up before arriving at the hospital for the surgery. Besides, you should shower and wash your hair on the night before or on the morning of the surgery.
- If you smoke, the surgeon will ask you to stop smoking for a while before the procedure.
- You will need to fast for at least six hours prior to the surgery. However, you can take your antiepileptic medicines as usual.
- If you agree to the procedure, your doctor will ask you to sign an approval or consent form.
See Similar Category Medicines Here

How is amygdalohippocampectomy done?
Once you reach the hospital, the hospital staff will provide you with a hospital gown to wear. Subsequently, an MRI will be performed to assist in the surgery. An intravenous line will be inserted in a vein in your hand to provide you with essential fluids and medicines during the surgery.
In the operating room, an anesthesiologist will administer general anaesthesia to put you into deep sleep. A tube will be inserted into your bladder to drain out urine. The procedure involves the following:
- A person from the surgery team will position your head on the operating table using a three-pin fixation device.
- They will shave the area to be operated and clean it with an antiseptic solution.
- The surgeon will mark the area on your scalp to make an incision (cut) and numb the region using local anaesthetic medicines. The cut will be made on the marked area.
- Then, the surgeon will use a medical drill to make small holes in your skull. Subsequently, he/she will use a special saw to cut the bone and remove a part of the bone (bone flap).
- The surgeon will separate the thick outer tissue covering your brain to expose your brain.
- With the aid of a surgical microscope, he/she will access your brain and remove parts of hippocampus and amygdala using microsurgical instruments.
- Finally, the surgeon will close the separated outer covering of your brain, fixe plates to the bone flap, and close the incision on your scalp.
After the procedure, you will be observed for a while in the recovery ward before being moved to the intensive care unit. You may need to stay at the hospital for three to four days after the surgery. During your hospital stay, you can expect the following:
- You will be kept in the intensive care unit to monitor your condition. A nurse will give you some medicines to reduce the swelling in your brain.
- A brain intracranial pressure device and an external ventricular drain may be used to monitor your brain pressure and remove extra fluids from your brain. They will be removed within a few days.
- Once your condition stabilises, you will be moved to the hospital room. You may require external oxygen supply for a few hours or days after surgery.
- A sequential compression device (sleeve-shaped) will be placed on your legs. An air compressor will pump air in and out of the sleeve to prevent the formation of blood clots.
- The tube inserted to drain out urine will be removed the next day.
- The hospital staff will raise the head of your bed to prevent swelling in your head and face.
- A specialist will visit you during your stay and teach some breathing exercises to help you breathe freely and prevent pneumonia.
- You will be encouraged to get out of the bed and move around soon as you can after the surgery.
How to care for yourself after amygdalohippocampectomy?
Once you reach home, you will need to take the following care:
- Keep the operated area dry. You may be allowed to wash your hair once the stitches are removed. However, avoid vigorous brushing or shampooing. Also, refrain from wearing a wig until the incision has healed completely.
- Do not lift heavy objects for several weeks.
- You should gradually increase your physical activity. Start with short walks during the initial few days and increase your pace and distance slowly over the next few days.
- You may experience severe headache while coughing and deep breathing. The surgeon may prescribe some medicines for the same. Take them as directed.
- Make sure to practise the breathing exercises taught at the hospital regularly
- Resume driving only after consulting with the surgeon.
When to see the doctor?
Contact the surgeon if you experience any of the following symptoms:
- Vision changes
- Fever
- Pain, bleeding, swelling, or redness around the operated area
- Weakness in the arms or legs
- Deficits in language
- Blood in sputum (mucus that is coughed up from the trachea, the lower airways)
- Excessive sleepiness
- Problems with body movement
- Confusion
- Anxiety
- Chest pain
- Difficulty breathing
What are the possible complications/risks of amygdalohippocampectomy?
The surgery carries the following risks:
- Infection
- Excessive bleeding
- Mood difficulties
- Vision problems
- Memory and language impairment
- No improvement in symptoms
- Risks of anaesthesia such as lung infection, confusion, stroke, and heart attack

When to follow up with your doctor after an amygdalohippocampectomy?
You will have a follow-up meeting with the neurologist (a medical expert who treats conditions related to the nervous system) and your surgeon eight to 12 weeks after an amygdalohippocampectomy. Your surgeon will ask you to undergo memory tests and an MRI three to four months following the procedure.
Additionally, you will have to visit a neuropsychologist (a psychologist who specialises in understanding the relationship between the physical behaviour and brain) and undergo another EEG or MRI one year after this surgery.
Disclaimer: The above information is provided purely from an educational point of view and is in no way a substitute for medical advice by a qualified doctor.
Surgery Cost In Your City

References
- Spencer D, Burchiel K. Selective amygdalohippocampectomy. Epilepsy Res Treat. 2012;2012:382095. PMID: 22957229.
- Cleveland Clinic [Internet]. Ohio. US; Temporal Lobe Seizures
- Panayiotopoulos CP. The Epilepsies: Seizures, Syndromes and Management. Oxfordshire (UK): Bladon Medical Publishing; 2005. Chapter 12, Symptomatic and Probably Symptomatic Focal Epilepsies: Topographical Symptomatology and Classification
- MHealth [Internet]. University of Minnesota. US; Selective Amygdalohippocampectomy
- National Health Service [Internet]. UK; Having an operation (surgery)
- Hernandez A, Sherwood ER. Anesthesiology principles, pain management, and conscious sedation. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 20th ed. Philadelphia, PA: Elsevier; 2017:chap 14
- dos Santos ARL, Mufarrej G, da Conceiçao PO, Cruz PLC, Cavalcanti DD, Chimelli L, et al. Surgical treatment of mesial temporal lobe epilepsy: selective amygdalohippocampectomy using Niemeyer's approach. Neurosurg Cases Rev. 2018;1:006
- Oxford University Hospitals [internet]: NHS Foundation Trust. National Health Service. U.K.; Epilepsy surgery







