Download App
Download App


What is an Iron test?
Iron tests refer to a group of tests that measure the level of iron reserves in body. Iron is essential for metabolic functions. An adult has an average of 3-5 grams of iron, of which two-thirds are present in haemoglobin. Iron tests detect both low and excess levels of iron in body.
The different types of iron tests are as follows:
- Serum iron: To determine the level of iron in serum.
- Transferrin: Iron is transported in the body by transferrin. Approximately, 33% of transferrin is normally saturated with iron.
- Total iron binding capacity/serum iron and transferrin: Total iron binding capacity (TIBC) is a measure of the total amount of iron combined with proteins in blood.
- Hypochromic cells in peripheral blood: The percentage of hypochromic cells (paler than normal RBCs) in a peripheral blood smear is determined.
- Serum ferritin: Serum ferritin levels indicate the amount of iron in the whole body.
Low levels of iron commonly lead to a condition called iron-deficiency anaemia. If the levels of iron are higher than normal, it is deposited in different parts of the body and leads to organ dysfunction. This condition may be caused by excess iron intake or increased absorption of iron.
- Why is an iron test performed?
- How do you prepare for an Iron test?
- How is an Iron test performed?
- Iron test results and normal range

Why is an iron test performed?
Iron tests are usually advised when symptoms of low iron are seen in patients. In the early stages of deficiency, symptoms are usually not seen, and iron reserves may be significantly low before the signs and symptoms appear. Decreased levels of iron may be seen in conditions such as anaemia, blood loss, burns, cancer, infection, inflammation, myocardial infarction and nephrosis.
The symptoms of low iron are
Iron accumulation in blood and tissues is indicated by abnormally high levels in conditions, such as
- Joint pain
- Fatigue
- Abdominal pain
- Damage in organs, such as the heart and/or liver
High iron levels occur due to conditions, such as acute liver damage, aplastic anaemia, haemochromatosis, haemolytic anaemia, hemosiderosis, lead poisoning, nephritis and polycythaemia.
How do you prepare for an Iron test?
The patient should avoid all solid foods 12 hours before the test. Any intake of food may interfere with test results; however, water is allowed. No iron supplements should be taken by the patient 24-48 hours before the test.
How is an Iron test performed?
An early morning blood sample is preferred, and it is taken from the patient’s arm. A volume of 5-10 mL is sufficient for the test. The whole test takes about 5 minutes. Possible but infrequent complications can be pain, light-headedness, bruising and local infection in the arm.
Iron test results and normal range
Laboratory levels of transferrin, iron and TIBC together provide the differential diagnosis of diseases, such as anaemia and assessment of iron-deficiency anaemia and helps evaluate thalassaemia, sideroblastic anaemia and hemochromatosis.
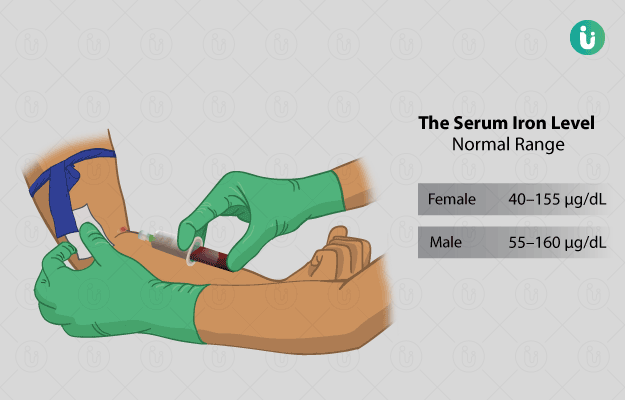
Normal results
- Iron:
- Adult men: 65-175 micrograms/decilitre (μg/dL) or 11.6-31.3 micromoles/litre (μmol/L)
- Adult women: 50-170 μg/dL or 9.0-30.4 μmol/L
- Children: 50-120 μg/dL or 9.0-21.5 μmol/L
- Newborns: 100-250 μg/dL or 17.9-44.8 μmol/L
- TIBC:
- Men: 250-450 μg/dL or 44.8-76.1 μmol/L
- Women: 250-450 μg/dL or 44.8-76.1 μmol/L
- Transferrin:
- Adults: 250-425 mg/dL or 2.5-4.2 g/L
- Children: 203-360 mg/dL or 2.0-3.6 g/L
- Newborns: 130-275 mg/dL or 1.3-2.7 g/L
- Transferrin (iron) saturation:
- Men: 10-50%
- Women: 15-50%
Abnormal results
Increased transferrin is observed in iron-deficiency anaemia, pregnancy and oestrogen therapy.
Decreased transferrin is found in microcytic anaemia associated with chronic disease, protein deficiency, loss from burns, malnutrition, chronic infection, acute liver disease, renal disease (nephrosis), genetic deficiency, hereditary atransferrinemia and hemochromatosis.
Decreased iron occurs in iron-deficiency anaemia, chronic blood loss, chronic diseases (eg, lupus, rheumatoid arthritis and chronic infections), pregnancy and progesterone birth control pills and inadequate iron absorption.
Increased iron occurs in haemolytic anaemia, thalassaemia, acute iron poisoning, iron overload and its syndromes, hemochromatosis, multiple transfusions, intramuscular iron, acute hepatitis, and liver damage.
Increased TIBC is found in iron deficiency, pregnancy, blood loss and hepatitis.
Decreased TIBC is observed in hypoproteinaemia, hemochromatosis, non–iron-deficiency anaemia, liver cirrhosis, nephrosis, thalassemia and hyperthyroidism.
The iron saturation index is increased in hemochromatosis, increased iron intake, thalassaemia, hemosiderosis and acute liver disease
The iron saturation index is decreased in iron-deficiency anaemia, malignancy, anaemia of infection and chronic disease.
Disclaimer: All results must be clinically correlated with the patient’s complaints to make a complete and accurate diagnosis. The above information is provided from a purely educational perspective and is in no way a substitute for medical advice from a qualified doctor.

References
- Drew P., Oxford Handbook of Clinical and Laboratory Investigation. Hematology. 4th ed. 2018 pp 244-247.
- Wintrobe's Clinical Hematology. 12th ed. Greer J, Foerster J, Rodgers G, Paraskevas F, Glader B, Arber D, Means R, eds. Philadelphia, PA: Lippincott Williams & Wilkins: 2009, pp 792-793, 826-827.
- Harmening D, Clinical Hematology and Fundamentals of Hemostasis, Fifth Edition, F.A. Davis Company, Philadelphia, 2009, pp 122-127.
- Wilson DD. Hill Manual of Laboratory and Diagnostic Tests. Iron. 2007 pp 341-342
- Frances TF. Manual of Laboratory and Diagnostic Tests. Iron Tests. 7th ed. 2003 pp 74-77.