


 Download App
Download App




Summary
Hemipelvectomy is a surgical procedure that involves the removal of the pelvic bone and sometimes the limb. The surgery is done for various conditions of the pelvis, for example, pelvic cancer. Extensive rehabilitative procedures, including the fitting of a prosthesis, are part of the recovery process of hemipelvectomy.
- What is hemipelvectomy?
- Why is hemipelvectomy recommended?
- Who can and cannot get hemipelvectomy?
- What preparations are needed before hemipelvectomy?
- How is hemipelvectomy done?
- How to care for yourself after hemipelvectomy?
- What are the possible complications/risks of hemipelvectomy?
- When to follow up with your doctor after a hemipelvectomy?

What is hemipelvectomy?
Hemipelvectomy is a complex surgery of the pelvis, that involves removal of the pelvic bone on one side, sometimes along with the limb on that side. It can be performed by external or internal technique. In external hemipelvectomy, half of the pelvic bone along with the leg on that side is amputated. In internal hemipelvectomy, the limb is preserved, and there is either complete or partial removal of the pelvis bone.
The hip bones form the bony structure of the pelvis along with two other bones (sacrum and coccyx), The pelvic cavity formed by these bones contains organs of the genitourinary tract such as the bladder and urethra, prostate gland and spermatic cords in males and uterus, fallopian tubes, ovaries, vagina and cervix in females; a large portion of the gastrointestinal tract; and nerves and blood vessels that supply to these organs and the limbs. During hemipelvectomy, it is necessary to identify and move these organs out of the way during the surgery to protect them.
This surgery is carried out in cases of tumours of the pelvic, hip, or thigh bone. It is performed to alleviate symptoms caused by uncontrollable malignancies or to prevent sepsis (the body’s reaction to infection leads to this life-threatening condition). A hemipelvectomy is also a treatment modality in cases of severe pelvic trauma.
Following surgery, the amputated part may be replaced with artificial prosthesis depending on factors such as age.
The best results from this surgical procedure can be achieved by a coordinated approach between various medical specialists such as surgeons, physiotherapists, occupational, and rehabilitative therapists.

Why is hemipelvectomy recommended?
A surgeon may recommend hemipelvectomy for the following conditions:
- A growth in pelvis accompanied by pain, inflammation, difficult bowel movements, etc., which diagnostic tests (such as a biopsy) have confirmed is a type of cancer that cannot be treated by chemotherapy or radiation, such as certain cancers of the bone or nerves or tumours of the pelvis identified at advanced stages.
- A tumour that presses on or infiltrates the sciatic nerve (the nerve that runs down from the lower back to both the legs).
- Severe injury to parts of hip bone and limb in an accident that requires amputation to prevent infection.
- Extreme trauma to the pelvic region, resulting in distortion and severe difficulty in maintaining function.
- Advanced pelvic infection (infection of pelvic tissue and muscles)
- Pelvic osteomyelitis (infection of the pelvic bone)
- Spinal cord injuries that cause pressure sores; however, surgery is rarely indicated in such instances.
- Other rare indications for a hemipelvectomy include kidney cancer, an advanced form of skin cancer called melanoma, bladder or rectal cancer, and other cancers that spread to the bone.
Who can and cannot get hemipelvectomy?
The surgery is not indicated in people who:
- Are very old
- Have a poor health condition and rapid metastases (spread of cancer)
Relative contraindications for which surgery can be performed, but caution is advised include tumours located at a considerable distance from the pelvic bone and a previous history of surgery that failed to remove a tumour.
What preparations are needed before hemipelvectomy?
Since this is a major surgery, some pre-operative procedures and tests are necessary. The following tests and preparations will be carried out before a hemipelvectomy:
- Your doctor will give you information about the procedure and its outcomes. You will be required to sign a consent form to give permission for the surgery.
- Tests will be carried out to check the fluid and electrolyte levels in your body. Imaging studies such as magnetic resonance imaging (MRI), computed tomography (CT) scan or x-ray of the pelvis will also be done.
- If you have any deficiencies such as anaemia, your doctor will give you medicines to correct them before the surgery.
- You will be put on an antibiotic a week before the surgery.
- You will be asked to have a clear, liquid diet for two days before surgery so your bowel get cleansed and there is less possibility of contamination of the wound.
- Your doctor may also advise you to use a mild enema the evening before the surgery to clean your bowel.
- A thorough cleaning of the vagina is recommended in females undergoing this surgery.
- An important step before this procedure is psychological counselling to deal with the possible consequences of the operation.
- Extra blood will be arranged to accommodate the need for blood transfusion during the procedure.
See Similar Category Medicines Here

How is hemipelvectomy done?
General anaesthesia (where you fall asleep during the procedure), spinal anaesthesia (a medicine is given in the spine to numb the lower part of the body) or a combination of both is given to during a hemipelvectomy based on the requirement of the individual.
You will be given an intravenous line through a vein for medicines. A Foley catheter will be inserted in your bladder to drain urine, and a nasogastric tube will be put into your stomach through your nose to provide nutrition. Both will be removed as needed after surgery.
Surgery is done in the following way:
External hemipelvectomy:
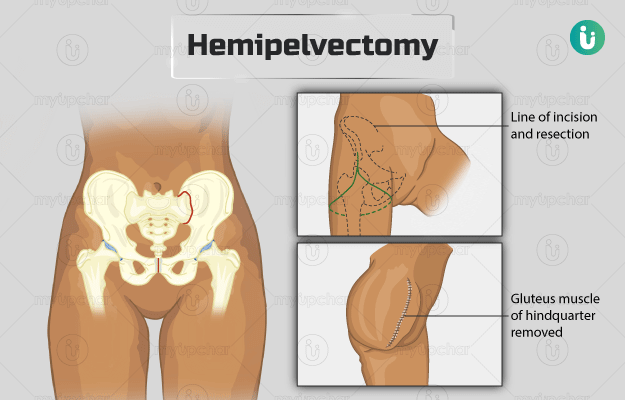
- The surgeon will make an incision in your skin from the top of your hip bone. The incision will bifurcate into two; one part of the incision will go to the joint in your pubic bones (pubic symphysis), and the other will go to the crease of your buttock, travel the entire length of the crease and come back to the starting point.
- The surgeon will then free your abdominal and pelvic muscles and your inguinal ligament (groin ligament) from of their attachments and cut and tie any major blood vessels in the area.
- He/she will retract your bladder into your pelvic cavity, and separate your pubic bones at the pubic symphysis (a joint that connects the two pubic bones).
- The surgeon will separate your remaining abdominal muscles and other muscles attaching your pelvic area to your body.
- Next, he/she will separate the bones from your sacroiliac joint (joint between the sacrum and ilium bones of the pelvis) and cut and tie the arteries and veins in the area. The nerve in this region will also be cut.
- Finally, the surgeon will detach the muscles of your pelvic floor and free your entire hindquarter.
- Before stitching back your muscles and skin in the area, the surgeon will make a new passage for your spermatic cord (which carries blood and lymphatic vessels, nerves that supply to the testicles, the tube that transports sperm, etc) by selectively stitching certain muscles in your pelvis and your abdomen.
Internal hemipelvectomy:
There are various methods of removing the hip bone. All these methods of resection (removal of part of the body) are such that important nerves and blood vessels are saved to ensure maximum function.
- For an internal hemipelvectomy, the surgeon will make an incision (cut) near your pubic symphysis.
- After penetrating deeper, he/she will separate any nerves, blood vessels and other structures from the tumour.
- Then, the surgeon will make a second incision along your femur (thigh bone).
- He/she will separate your gluteus muscles (muscles that make up the buttocks), and remove a part of the muscle along with the tumour.
- The surgeon will then separate your hip bone from the surrounding structures, and use an instrument called an oscillating saw to cut the affected part.
- Once all the affected area is removed, the surgeon will use electrocautery to stop bleeding. In electrocautery, a wire is heated by passing a current through it and the heated wire is then used to destroy tissue or in this case, stop bleeding,
- The removed tumour is then sent to a laboratory for further investigations.
- There are various modifications to this depending on the exact location of the tumour in order to minimise the damage to the surrounding structures. The types of internal resection based on the area removed are as follows:
- Type I: Removal of the iliac wing (the broadest part of the ilium)
- Type II: Removal of the area around the acetabulum (the socket in the hip joint that houses the end of the thigh bone)
- Type III: Removal of the pubic rami, the anterior-most part of the hip, the pubic bones.
- Type IV: Removal of the sacrum, the large, flat bone between the hip bones located below the lumbar vertebrae.
- The type of resections can be combined based on the extent of tumour to be removed.
The surgery may last between three and nine hours. After the surgery, you will most likely remain in the hospital care for about two weeks. Reconstruction of the hip and hemipelvis may be done based on the individual’s age, functional requirements of the extremity, personal expectations, and consideration for difficulties faced with prosthetics such as the difficulty in anchoring the prosthetic with a shoulder or waist strap.
After the surgery:
- You will be given oral medication for pain management, anticoagulant medicines like Coumadin for maintaining adequate international normalized ratio (INR) values to prevent blood clotting or haemorrhage, and antibiotics until the wound stops draining.
- As part of the recovery process, the medical team will monitor your heart health, kidney health, respiratory function, neurologic function, and electrolytes.
- To prevent wound infection and pressure sores due to a longer period in bed, the medical staff will ensure that the surgery site is clean.
- Usually, a physical therapist will start physical therapy at about 6 weeks after surgery. Your movement will be gradually increased from sitting up in bed to walking with assistance. You may be sent to a rehabilitation program to promote movements.
- A neuromuscular exam will be conducted to test for any problems.
- A psychiatry consultation may be arranged to help you cope with the loss of a limb.
- The types of prosthesis, the challenges of each, the training required, and the duration after which a prosthesis can be fit will be discussed with you.
How to care for yourself after hemipelvectomy?
Post-surgery recovery will require co-operation and assistance from your family members and caregivers.
During the recovery process, the medical and rehabilitation team will also educate you about the use of a wheelchair, crutch or any other such equipment.
Make sure that you regularly clean the wound as advised by your doctor. This would help prevent complications such as infection or necrosis (death of tissue).
When to see the doctor?
You should visit the doctor if you have:
- Symptoms of infection such as fever
- Phantom pain (sensation of pain from an amputated organ)
- Abnormal bone growth
- Skin abrasions from prosthesis use
- Swelling in the other leg
What are the possible complications/risks of hemipelvectomy?
The complications following the surgery are:
- Necrosis of the flap (death of the tissue of the flap)
- Wound infection
- Complete dependence on a wheelchair or a risk of being permanently bed-ridden
- Phantom limb pain
- There is also a chance that cancer may recur or spread to a different part of the body
- Loosening of the prosthesis

When to follow up with your doctor after a hemipelvectomy?
Your follow-ups will be scheduled at intervals of 3 weeks, 6 weeks, and 3 months after the surgery. During the visits, the doctor will check for postoperative complications, psycho-emotional changes such as altered body image, and the recurrence or spread of cancer.
Disclaimer: The above information is provided purely from an educational point of view and is in no way a substitute for medical advice by a qualified doctor.

References
- Cedars Sinai [Internet]: Cedars Sinai Medical Center. Los Angeles. US; Surgical Options: Hemipelvectomy
- Malawer MM, Sugarbaker PH. Musculoskeletal cancer surgery. 2001 ed. Dordrecht: Springer; 2001. Chapter 20, posterior flap hemipelvectomy; p. 319–336.
- Baliski CR, Schachar NS, McKinnon JG, Stuart GC, Temple WJ. Hemipelvectomy: a changing perspective for a rare procedure. Can J Surg. 2004 Apr;47(2): 99–103. PMID: 15132462.
- D'Alleyrand, Lewandowski LR, Forsberg JA, Gordon WT, Fleming ME, Mullis BH, et al. Combat-related hemipelvectomy: 14 cases, a review of the literature and lessons learned. J Orthop Trauma. 2015 Dec;29(12):e493–e498.
- Wedemeyer C, Kauther MD. Hemipelvectomy- only a salvage therapy?. Orthop Rev (Pavia). 2011 Mar 17;3(1):e4. PMID: 21808716.
- Chan J, Virgo KS, Johnson FE. Hemipelvectomy for severe decubitus ulcers in patients with previous spinal cord injury. Am J Surg. 2003 Jan;185(1):69–73. PMID: 12531450.
- Schwartz AJ, Eckardt JJ, Beauchamp CP. Internal hemipelvectomy for musculoskeletal tumors— indications and options for reconstruction. US Oncology & Hematology, 2011;7(2):123–5.
- Rudert M, Holzapfel BM, Pilge H, Rechl H, Gradinger R. [Partial pelvic resection (internal hemipelvectomy) and endoprosthetic replacement in periacetabular tumors]. Oper Orthop Traumatol. 2012 Jul;24(3):196–214. PMID: 22743633.
- Ariel IM, Hark FW. Disarticulation of an innominate bone (hemipelvectomy) for primary and metastatic cancer. Ann Surg. 1949 Jul;130(1):76–99. PMID: 17859415
- Lackman RD , Crawford EA, Hosalkar HS, King JJ, Ogilvie CM. Internal hemipelvectomy for pelvic sarcomas using a T-incision surgical approach. Clin Orthop Relat Res. 2009 Oct;467(10):2677–84. PMID: 19381740.
- BANKS SW, COLEMAN S. Hemipelvectomy: surgical technique. J Bone Joint Surg Am. 1956;38-A(5):1147-1155. PMID: 13367092
- Wu KK, Guise ER, Frost HM, Mitchell CL. The surgical technique for hindquarter amputation. A report of 19 cases. Acta Orthop Scand. 1977;48(5):479-486. PMID: 596143.
- Mat Saad AZ, Halim AS, Faisham WI, et al. Soft tissue reconstruction following hemipelvectomy: eight-year experience and literature review. ScientificWorldJournal. 2012;2012:702904. doi:10.1100/2012/702904.
- Granda-Cameron C, Hanlon AL, Lynch MP, Houldin A. Experience of newly diagnosed patients with sarcoma receiving chemotherapy. Oncol Nurs Forum. 2011;38(2):160-169. PMID: 21356654.
- Mayerson JL, Wooldridge AN, Scharschmidt TJ. Pelvic resection: current concepts. J Am Acad Orthop Surg. 2014;22(4):214-222. PMID: 24668351.
- National Cancer Institute [Internet]. Bethesda (MD): U.S. Department of Health and Human Services; Adult Soft Tissue Sarcoma Treatment (PDQ®)–Health Professional Version
- Beck LA, Einertson MJ, Winemiller MH, DePompolo RW, Hoppe KM, Sim FF. Functional outcomes and quality of life after tumor-related hemipelvectomy. Phys Ther. 2008;88(8):916-927. PMID: 18535089.
- BinitieO, Alvero C, Letson GD. Musculoskeletal bone and soft tissue tumors. In: Maagee DJ, Zachazewski JE, Quillen WS, Manske RC. Pathology and intervention in musculoskeletal rehabilitation. 2nd ed. Philadelphia: Elsevier Saunders; 2016; p. 1175–1194.
- WATKINS AL. Rehabilitation after hemipelvectomy. JAMA. 1962;181:793-794. PMID: 14005243.
- Apffelstaedt JP. Complications and outcome of external hemipelvectomy in the management of pelvic tumors. Annals of surgical oncology. 1996 May 1;3(3):304-9.
- White EA, Learch TJ, Matcuk G, Gottsegen C, Menendez LR, Ahlmann ER, et al. Review of hemipelvectomy endoprostheses: indications and imaging findings. Appl Radiol. 2013 Jan; 42(6):23A–23J.
- Ham SJ, Schraffordt Koops H, Veth RP, van Horn JR, Eisma WH, Hoekstra HJ. External and internal hemipelvectomy for sarcomas of the pelvic girdle: consequences of limb-salvage treatment. Eur J Surg Oncol. 1997;23(6):540-546. PMID: 9484927







