


 Download App
Download App





Summary
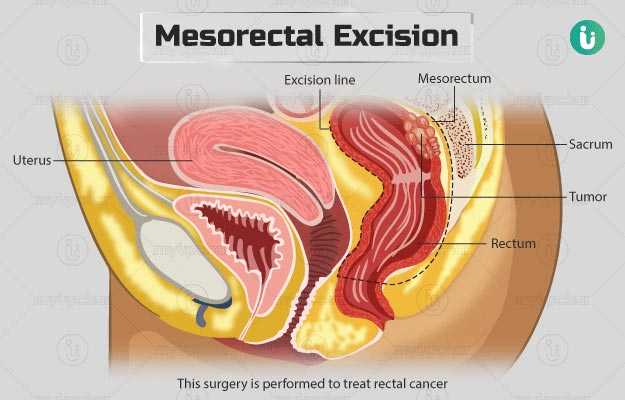
Mesorectal excision is performed to treat rectal cancer. In this surgery, the affected portion of the rectum (end part of the large intestine) is removed and the rest of the rectum is then connected to the intestine. The procedure can be performed by an open or laparoscopic technique and usually takes about four hours. Your doctor will perform different tests before the surgery to assess your overall health and will ask you to discontinue certain medicines that may lead to complications during or after the procedure.
After the surgery, you will be in the hospital for about three to six days. Your bowel movements will change due to the surgery, but over time they will improve. You will be asked to avoid doing any strenuous activities while you are healing. A follow-up visit will be scheduled about one to three weeks after your discharge to remove your stitches.
- What is mesorectal excision?
- Why is mesorectal excision recommended?
- Who can and cannot get mesorectal excision?
- What preparations are needed before mesorectal excision?
- How is mesorectal excision done?
- How to care for yourself after mesorectal excision?
- What are the possible complications/risks of mesorectal excision?
- When to follow up with your doctor after mesorectal excision?

What is mesorectal excision?
Mesorectal excision (ME) is the preferred method for the treatment of rectal cancer.
Rectum is a part of your digestive system. Once nutrients from the food are absorbed in the small intestine, the waste material left passes through the large intestine/colon, where some water is absorbed from it. The remaining portion is stored in the rectum (last part of the large intestine) until it is eliminated from the anus (back passage).
Mesorectal excision involves the removal of the affected part of the rectum along with the nearby lymph glands and blood vessels. The colon is then reconnected to the remaining rectum with the help of staples or stitches. The point of connection is known as an anastomosis.
You will have regular bowel movements after healing. The healing of the rectum is slow, and hence a temporary stoma (an opening on the abdomen through which stools can exit and collect into a pouch placed over the stoma – ileostomy) may be created. This diverts stools from the connection and gives the rectum time to heal. The ileostomy is generally reversed, and the stoma closes in a few months after ME.
Some people may have permanent stoma when the rejoining of the colon and rectum is not possible, or they may choose to have the stoma due to poor bowel control.
Why is mesorectal excision recommended?
The ME can be used for the treatment of the following conditions:
- Certain stage I rectal cancers (presence of cancer only in the inner layers of the rectum)
- Majority of stage II (spread of cancer to all the layers of the rectum) and III (cancer spread to the nearby lymph nodes) rectal cancers located in the upper region of the rectum
Some symptoms of rectal cancer include:
- Blood in stools
- Diarrhoea
- Constipation
- Reduced diameter of stools (pencil-thin)
- Tiredness
- Pelvic pain or abdominal pain
- Unexplained weight loss
- Tenesmus (a feeling to pass stools when you do not need or are unable to pass them)
Are you also troubled by obesity and are not able to lose weight even after a lot of efforts, then start using myUpchar Ayurveda Medarodh Weight Control Tablet today and control your weight.
Who can and cannot get mesorectal excision?
Mesorectal excision cannot be performed if cancer has spread to the surrounding tissue in the pelvis or anal sphincter (muscles that control the passing of stools).
What preparations are needed before mesorectal excision?
You will need the following preparations before the surgery:
- Share the following details with your doctor:
- Your medical history
- If you have any allergies or implanted medical devices such as a pacemaker
- All the medicines that you take, including any supplements, minerals, vitamins, and non-prescription medicines
- Your doctor will conduct a physical examination, and will order the following tests:
-
- Blood tests
- Electrocardiogram (ECG)
- Chest X-ray
- Digital rectal examination (to look for the presence of any rectal masses)
- Sigmoidoscopy (a procedure to examine the rectum)
- Endorectal ultrasound (to determine the amount of tumour penetration through the wall of the rectum)
- Computed tomography (CT) scan
- You will be asked to discontinue the use of alcohol and tobacco once the surgery is planned. Additionally, you will need to discontinue certain medicines like nonsteroidal anti-inflammatory drugs (NSAIDs), vitamin E, and supplements.
- Do not have any food or water after midnight before the surgery.
- Make sure to bring along a companion as you will not be able to drive yourself back home.
- You will have to sign an approval form if you agree to the procedure.
How is mesorectal excision done?
Once admitted to the hospital, you will first be given an enema to clear your bowel. After this, the medical staff will provide you with a hospital gown, and you will be taken to the operating room.
You will lie on an operating table and wear compression boots to help the circulation in your legs. A catheter (tube) will be inserted in your bladder to drain urine. Different devices to check your heart rate, oxygen levels, and blood pressure will be attached to your body to monitor your vitals throughout the procedure. An intravenous (IV) line will be started in your arm or hand. This will be used to give you fluids and medications.
You will be administered with general anaesthesia (a sleep-inducing medicine) and the surgery will be performed either by an open or laparoscopic method.
Open surgery involves the following steps:
- The surgeon will make an incision (cut) from your belly button to pubic area.
- He/she will free your colon, ureter, nerves and the blood vessels of your reproductive organs.
- Then, the surgeon will cut the blood vessels that supply blood to your rectum.
- He/she will make a cut on your rectum to reach and remove the tumour along with a margin of healthy tissue. The surgeon will also remove the mesenteric tissue surrounding the cancerous tissue.
- Then, he/she will attach your rectum and colon with either sutures or staples, re-place all your organs in through the opening and close your abdomen.
- If needed, a temporary ileostomy may be done, in which a part of the intestine is brought out through an opening (a stoma) on the top of your abdomen. A pouch will be connected to the stoma to collect stools that pass out through your body. Ileostomy allows the rectum to heal.
The laparoscopic surgery is performed by making multiple small incisions (instead of one large one) on the abdomen. The surgeon will insert surgical tools and a tiny camera into your abdomen to perform this procedure.
It takes around four hours to complete this procedure. After the surgery, the medical staff will move you to the recovery room. You will have an oxygen mask, and pain medicines will be administered to you to make you feel comfortable before shifting you to the hospital room. The urinary catheter will be removed as soon as possible.
You may be able to drink and eat as usual after the surgery. The hospital staff will encourage you to get out of bed and move around as early as possible.
You will be discharged three to six days after the surgery. However, this may vary based on your condition.
How to care for yourself after mesorectal excision?
Once you reach home, you will need to take care of yourself in the following manner:
- Bowel movements: Since a part of your rectum is removed, your bowel movements will be different after the surgery. Over time, you will notice an improvement. Some tips to help in improving your bowel movements are as follows:
- Counselling: If you need to talk to anyone and express your feelings after the surgery, you may seek counselling and support.
- Medication: You may need painkillers to help control your pain and perform your daily activities.
- Bathing: You may be able to take a shower daily, and wash your incision gently with a mild soap. Make sure to pat the area dry gently after your bath. Avoid using hot tubs, bathing in a tub, and swimming till the follow-up visit.
- Caring for your ileostomy: If you have an ileostomy after the surgery, you will need to empty your pouch when it is about half full. Check for any leakage in the pouch, and change it every three to five days.
- Activities: Avoid doing any strenuous activities, playing sports, and carrying weights for about six weeks after the surgery.
- Driving: Your doctor may allow you to resume driving once you don't have any pain, i.e., about two weeks after the surgery. Do not drive if you are on pain medication.
- Wound care: Do not apply any ointments and creams on the incision. Avoid any clothes that may irritate the skin around the operated area.
- Avoid using hot tubs, bathing in a tub, and swimming till the follow-up visit.
When to see the doctor?
You may need to immediately visit your doctor if you observe any of the following signs:
- Fever
- Redness, swelling, or pain at the surgery site
- Discharge of bowel contents or pus
- Bleeding from the rectum
- Abdominal pain
- Nausea and vomiting
- Difficulty in urinating
- Dehydration symptoms, such as dizziness while standing, excessive thirst, headache, dry skin and dry mouth.
- No output in the ileostomy for two hours
What are the possible complications/risks of mesorectal excision?
Some of the potential complications are as follows:
- Leakage in the anastomosis
- Cardiopulmonary complications
- Bleeding in the abdomen
- Infection
- Deep vein thrombosis
- Inability to control stool and urine
- Vaginal dryness
- Problems associated with erection and ejaculation
- Ileus (temporary inability to pass bowels)
- Complications due to anaesthesia, including nausea, slow breathing, and allergic reaction

When to follow up with your doctor after mesorectal excision?
The follow-up visit will be scheduled seven to 20 days after your discharge to remove sutures or staples. If you have had a temporary ileostomy, another surgery will be done in a few months’ time to close the ileostomy.
Disclaimer: The above information is provided purely from an educational point of view and is in no way a substitute for medical advice by a qualified doctor.
Surgery Cost In Your City

Doctors for Mesorectal excision

Dr. Abani Kanta Nanda
Oncology
11 Years of Experience

Dr. Anil Gupta
Oncology
6 Years of Experience

Dr. Akash Dhuru
Oncology
10 Years of Experience

Dr. Anil Heroor
Oncology
22 Years of Experience
References
- St. Helens and Knowsley Teaching Hospitals [Internet]. NHS Foundation Trust. National Health Service. UK; Patient Information for Total Mesorectal Excision
- Memorial Sloan Kettering Cancer Center [Internet]. New York. US; About Your Low Anterior Resection Surgery
- American Cancer Society [Internet]. Georgia. US; Surgery for Rectal Cancer
- Cedars Senai [Internet]. California. US; Colon and Rectal Cancers
- American Society of Colon and Rectal Surgeons [Internet]. Illinois. US; Rectal Cancer
- OncoLink: University of Pennsylvania [Internet]. US; All About Rectal Cancer
- Tjandra JJ, Clunie GJA, Kaye AH, Smith J. Textbook of surgery. 3rd ed. Massachusetts: Blackwell publishing; 2006. Chapter 24, colorectal cancer and adenoma; p. 191–210.
- Mchir RN, Baker D, Goddard N. Kirk’s general surgical operations. 6th ed. Edinburgh: Churchill Livingstone; 2013
- Moffitt Cancer Center [Internet]. Florida. US; Traditional vs. Robotic Low Anterior Resection Surgery
- UCSF Health [Internet]. University of California San Francisco. California. US; After low anterior resection for treatment of rectal cancer
- Michigan Medicine [internet]. University of Michigan. US; Instructions following abdominal surgery
- Phang PT. Total mesorectal excision: technical aspects. Can J Surg. 2004 Apr;47(2):130–137. PMID: 15132469.
- Feroci F, Vannucchi A, Bianchi PP, Cantafio S, Garzi A, Formisano G, Scatizzi M. Total mesorectal excision for mid and low rectal cancer: Laparoscopic vs robotic surgery. World J Gastroenterol. 2016 Apr 7;22(13):3602-10. PMID: 27053852.







