


 Download App
Download App





Summary
Oesophagectomy is an operation carried out to treat oesophagus (food pipe) cancer, ulcers or to remove damaged oesophagus due to an accident or injury. It is a major operation, which takes a few weeks to recover.
After the operation, you will have to take proper care of the wound and follow the dietary advice given. In case you find any abnormal symptoms, contact your healthcare provider immediately.
- What is oesophagectomy?
- Why is oesophagectomy recommended?
- Who can and cannot get oesophagectomy?
- What preparations are needed before oesophagectomy?
- How is oesophagectomy done?
- How to care for yourself after oesophagectomy?
- What are the possible complications/risks of oesophagectomy?
- When to follow-up with your doctor after an oesophagectomy?

What is oesophagectomy?
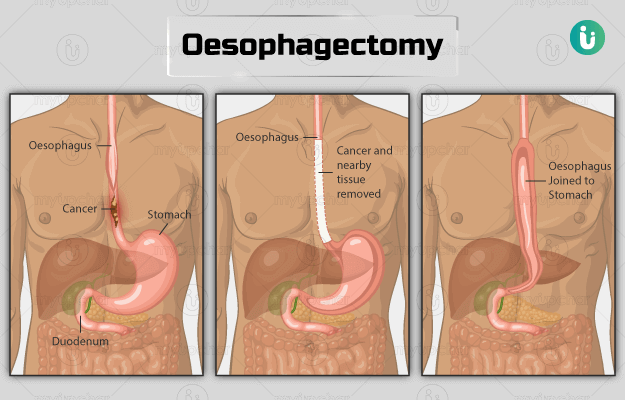
Oesophagectomy is a surgical procedure in which either a part of or the whole oesophagus is removed. The oesophagus or gullet is a long muscular tube that transports food from the mouth to the stomach. It has a valve at the lower end that prevents the backflow of food and fluid from the stomach into the oesophagus (reflux).
Oesophagectomy is done for conditions like oesophageal cancer, ulcers, and injuries that damage the food pipe and cause discomfort (like swallowing acid) and cannot be treated by another method.
Surgery is the only treatment for oesophagus cancer. It may often be done along with other therapies like chemotherapy or radiation.
After removing the cancerous part, the rest of the oesophagus is connected to the stomach.

Why is oesophagectomy recommended?
Oesophagectomy may be recommended in people with the following conditions :
- Oesophageal cancer.
- Achalasia after trying other treatment options. [Achalasia is a rare disease of oesophagus which makes it difficult for food/liquid to pass from mouth to stomach)
- Severely damaged oesophagus due to swallowing acids, acid reflux, or during any other medical operations.
- Have a growth or an ulcer (other than cancer), which needs to be removed for causing problems. Oesophagal ulcers can present with chest pain, nausea, dysphagia, regurgitation and water brash.
The following symptoms indicate oesophageal cancer:
- Difficulty in swallowing
- Weight loss
- Indigestion, heartburn or cough that does not get better
- Food coming back up
- Pain in the throat or chest
- Hoarseness of the voice
- Coughing up blood or vomiting blood
- Breathlessness, tiredness
- Pale skin
- Loss of appetite
- Pain or discomfort in the upper stomach, back, or chest
Troubled by obesity? Failed to lose weight? Now control weight easily by myUpchar Ayurveda Medarodha Weight Control Tablet. Get started today and take steps towards a healthy life.
Who can and cannot get oesophagectomy?
Contraindications to the techniques used for oesophagectomy are:
- Ivor-Lewis oesophagectomy: This procedure is not recommended for high oesophageal carcinomas located across 20 cm of the incisors. It is relatively contraindicated in people who have undergone a previous right thoracotomy (incision into the chest wall) because of postoperative adhesion.
- Minimally- invasive oesophagectomy: The contraindications for this surgery include:
- Extensive pleural adhesions (scar tissue in the lungs)
- Impaired circulatory function that prevents single-lung ventilation
- Tumour infiltrating structures, a coexisting serious medical condition (diabetes mellitus, liver cirrhosis, or chronic renal failure)
- People refusing to undergo this surgery or those who have received radiation in the mediastinum, the cavity that contains organs such as the heart and parts of the oesophagus and trachea.
- Transhiatal oesophagectomy: Contraindications for this procedure include:
- Tracheobronchial, intra-abdominal, and mediastinal structures invasion
- Advanced physiologic age and weakness
- Stage IV disease
- Prohibitive comorbidities
What preparations are needed before oesophagectomy?
You need to be healthy (fit enough) before this operation. The following preparatory steps will need to be taken before the surgery:
- Stop smoking immediately to reduce the risk of breathing problems and chest problems after the operation. You should not use electronic cigarettes or nicotine patches as they may also lead to complications.
- Exercise regularly by walking, gardening, cycling, dancing, golf, or swimming to keep yourself fit.
- Maintain a healthy diet or take a dietician’s advice if required.
- A healthcare provider will take your health history and perform a physical exam. History of surgery to the stomach or colon will be asked for, as previous abdominal surgery may affect reconstruction after removal of the oesophagus.
- You need to get blood tests done, such as complete blood count (CBC), liver function tests, and blood clotting profile.
- You will need to get heart and lung function tests done to ensure you are fit for the surgery. A physiotherapist will teach you special breathing and coughing exercises to clear your lungs.
- A nutritional assessment may be done to see your food intake and weight. You may need nutritional supplements, intravenous feeding, and a feeding tube for a few days before and after the operation to enhance your nutrition and health.
- If your immune system is weakened due to poor nutrition, then you may need antibiotics to prevent infections.
- Cardiopulmonary exercise test (CPET or CPEX test) will be performed by an anaesthetist, which involves evaluating heart and lung function while exercising on a cycling bike.
- An echocardiogram may be required, which indicates the functioning of the heart and any problems with heart valves.
- Avoid eating anything 6 hours before the surgery.
The following diagnostic tests may also be done before the surgery:
- Endoscopy: Here, your oesophagus and stomach will be examined by a flexible camera to locate the cancer and show where it is growing.
- Computed tomography (CT) scan: It is a body scan that shows the size, location, and spread of cancer using X-rays.
- Positron emission tomography (PET) scan: A body scan that uses radioactive tracers to look for the spread of cancer to other body parts.
- Staging laparoscopy: It is a keyhole surgery to examine the stomach to check the viability of surgery and the spread of cancer. The different stages of oesophageal cancer are.
- Stage 0: Indicates the presence of severely abnormal cells in the inner lining of the oesophagus.
- Stage 1: Indicates that the cancer is still limited to the inside of the oesophagus wall.
- Stage 2: This stage is divided in to stage 2A and 2B. Stage 2A means cancer has spread to the lining outside the oesophagus. Stage 2B means cancer has spread to the muscle layer and to one or two nearby lymph nodes.
- Stage 3: It is divided into stage 3A, 3B, and 3C.
- Stage 3A: Cancer has grown either into the tissue covering of the lungs (pleura), a muscle at the base of the rib cage (diaphragm), the external covering of the heart (pericardium), or the membrane covering the oesophagus and spread to one or two adjacent lymph nodes.
- Stage 3B: Cancer has spread into the membrane covering the oesophagus and to three to six lymph nodes, but nowhere else.
- Stage 3C:
- Cancer has spread to the parts similar to stage 3A and to up to seven nearby lymph nodes.
- It may also spread to nearby structures like the windpipe, a spinal bone or the aorta (major blood vessel) and any number of local lymph nodes. Evidence does not show that it has spread to anywhere else.
- It can be of any size and spread to seven or more lymph nodes, but with no evidence that it has spread to another part of the body.
- Stage 4: It means the cancer is advanced and has spread to other body parts, such as the liver or lungs.
See Similar Category Medicines Here

How is oesophagectomy done?
You may expect the following things on the day of the surgery:
- A surgeon and anaesthetist will meet you before the surgery and the surgeon will explain the procedure.
- You will be asked to sign a consent form to allow the surgeon to perform the procedure.
- An intravenous (IV) drip will be placed in your arm.
- If you are diabetic, you will be given an infusion of insulin and glucose to control your blood sugar.
- You will be provided with a pair of stockings to wear and given blood-thinning medicine to reduce the risk of blood clots in your veins.
- You will be asked to change into a theatre gown and remove any jewellery.
- A healthcare practitioner will give you an epidural, i.e., a fine needle inserted into the back near the spinal cord to give you painkillers.
- An injection will be given to you through the IV to make you fall asleep.
In this surgery, the upper portion of the stomach is commonly removed so that the position of the stomach will be higher than before, which will help in swallowing. The surgery basically involves the following steps:
- The affected part of the oesophagus is removed and the stomach is reshaped, allowing it to be drawn up into the neck or chest and remaining oesophagus and stomach are joined.
- The lymph nodes affected by cancer are removed
- A temporary tube for feeding is inserted into the jejunum (small bowel)
Oesophagus can be accessed through the neck, chest, or stomach. However, the approach chosen for surgery depends on the location of cancer. The types of oesophagectomy are:
- Ivor-Lewis oesophagectomy (transthoracic oesophagogastrectomy): For this procedure, a cut will be made in the centre of your stomach and along the side of your body, towards your back to remove the tumour.
- Transhiatal oesophagectomy: For this procedure, the affected part of the oesophagus will be removed by making two cuts, one in the neck and one in the stomach to remove the tumour. The stomach will be joined to the oesophagus through the neck incision.
- McKeown oesophagectomy (3-hole oesophagectomy): For this surgery, the cuts will be made in your abdomen, right upper back, and neck.
- Minimally invasive oesophagectomy: For this procedure, several small cuts will be made in your abdomen and back below your shoulder. A laparoscope and surgical instruments will be put into your abdomen through these cuts to remove the tumour. The surgeon may use their hands or a robot to control the tools.
After the surgery is completed, you will wake up in the ICU. You will be closely monitored and then moved to a surgical ward with several tubes attached. The next steps are mentioned below:
- You will be provided fluid through your IV line till you can eat and drink.
- When you wake up:
- A nasogastric tube (passes down the stomach through the nose to drain air and fluid from the stomach in the chest) will be in place. On the fourth day, if a small quantity of fluid is draining from it, then the tube will be removed. You will be able to drink freely.
- A urinary catheter will be in place in your bladder to drain urine. It also helps check renal function after the surgery.
- Local anaesthetic catheters will be in place next to the incisions. These are used to deliver pain killers to the incisions directly.
- A drain will be placed in the stomach to drain the fluid from there.
- All the drains will be removed by the sixth day.
- You will also have a feeding tube (jejunostomy) for the first five to seven days as you are not able to eat or drink via the mouth.
- You will feel some pain or discomfort in the operated area, which will be controlled by giving pain-relieving drugs.
- Move around as early as possible to prevent chest infections.
- About five days after the surgery, a special drink will be given, and you will have an X-ray to check if the join inside has sealed and ensure that there is no leakage. You cannot drink until you take this test.
- Usually, patients are allowed to go home two weeks after this surgery.
How to care for yourself after oesophagectomy?
You should take the following care after the surgery.
- Pain: You may feel some pain for some time after the surgery. Your doctor will give you pain killers to help relieve the pain.
- Wound care: You may feel unusual sensations (numbness, itching, or tingling), light pulling near the stitches as the wound heals, and a slight hard lumpy feeling as new tissue forms. Avoid pulling away any scabs as they help in protecting the new tissue and act as a natural dressing. They will wear off on their own.
- Bath and shower: Do not soak in a bathtub unless your doctor allows you to. Ensure that the wound is dry.
- Diet: A dietician will assist you with your diet before you get discharged. You will be advised to have a ‘fork-mashable’ diet for the first few weeks before going to a usual diet. You may experience weight loss, not feel hungry, have difficulty in swallowing, reflux at night, have nausea and dumping syndrome (when food in stomach empties very fast into the small intestine). Follow these tips to avoid the symptoms:
- Take frequent small meals.
- Chew your food properly and take small bites. Eat moist, soft foods as they are easier to swallow and digest.
- Avoid carbonated drinks, caffeine, alcohol, tomato products, citrus, spicy or fried foods, sticky foods like banana, and doughy bread.
- Avoid too cold or hot foods.
- Sweets should be taken at the end of the meal, as eating them first can lead to low blood glucose.
- Do not chew tobacco or gum.
- Do not eat at a minimum of two hours before you go to sleep.
- Sit straight while eating as gravity helps to move the food down.
- Limit your fluids to half a cup with meals and one cup with snacks. It will help with dumping syndrome and feeling full.
- Activity: You may feel tired at first, but it will improve over the weeks. You can do breathing exercises advised by the physiotherapist in the hospital. Gradually increase your activities over the weeks. Gentle exercise will facilitate your energy levels and appetite. Avoid lifting heavy weights or pushing or pulling for the first eight weeks or till the wound is completely healed.
- Driving: You won’t be able to drive until six to eight weeks after the surgery.
When to see the doctor?
You should contact your doctor if you find the following symptoms after the surgery:
- Difficulty in swallowing
- Pain in the chest or back
- Weight loss
- Change in the body that worries you
What are the possible complications/risks of oesophagectomy?
The possible complications after an oesophagecotmy include:
- Wound, urine, or chest infection
- Skin infection around any tubes
- Bleeding
- Blood clots: deep vein thrombosis (blood clotting in the vein), pulmonary embolus (blockage of an artery in the lungs)
- Swelling of the legs, sometimes the abdomen
- Heart problems
- Anastomotic leak – any new join leakage
- Injury to the structures near the oesophagus
- Chyle (a milky fluid made from the digestion of fatty foods) leak
- Stomach not emptying
- Delayed feeding

When to follow-up with your doctor after an oesophagectomy?
Your first follow-up will be in two to four weeks after getting discharged.
Disclaimer: The above information is provided purely from an educational point of view and is in no way a substitute for medical advice by a qualified doctor.
Find Gastroenterologist in cities
- Gastroenterologist in Gurgaon
- Gastroenterologist in Bangalore
- Gastroenterologist in Chennai
- Gastroenterologist in Jaipur
- Gastroenterologist in Ahmedabad
- Gastroenterologist in Noida
- Gastroenterologist in Mysore
- Gastroenterologist in Visakhapatnam
- Gastroenterologist in Hyderabad
- Gastroenterologist in Pune
Surgery Cost In Your City

Doctors for Oesophagectomy

Dr. Rishabh Gupta
Gastroenterology
6 Years of Experience

Dr. Paramjeet Singh.
Gastroenterology
10 Years of Experience

Dr. Nikhil Bhangale
Gastroenterology
10 Years of Experience

Dr Jagdish Singh
Gastroenterology
12 Years of Experience
References
- Hull University Teaching Hospitals [internet]: NHS Foundation Trust. National Health Service. U.K., Oesophagectomy
- UW Health: American Family Children's Hospital [Internet]. Madison (WI): University of Wisconsin Hospitals and Clinics Authority; Esophagectomy
- Cancer Research UK [Internet]. London. UK; Symptoms of oesophageal cancer
- National Health Service [internet]. UK; Symptoms : oesophageal cancer
- Kim S H, Lee K S, Shim Y M, Kim K, Yang P S, Kim T S. Esophageal resection: indications, techniques, and radiologic assessment. Radiographics . 2001 Sep-Oct;21(5):1119-37. PMID: 11553820.
- Kawakubo H, Takeuchi H, Kitagawa Y. Current status and future perspectives on minimally invasive esophagectomy. Korean J Thorac Cardiovasc Surg. 2013 Aug; 46(4): 241– 248. PMID: 24003404.
- Iowa Head and Neck Protocols: University of Iowa Healthcare [Internet]. University of Iowa Carver College of Medicine: University of Iowa. US; Esophagectomy: Transhiatal—Laparotomy with Cervical Anastomosis
- Canadian Cancer Society [internet]. Toronto. Canada; Surgery for esophageal cancer
- The Norfolk and Norwich University Hospitals NHS Foundation Trust [Internet]. National Health Service. UK; Your Preparation for Oesophagectomy
- NHS Highland [Internet]. National Health Service. UK; Oesophagectomy
- Memorial Sloan Kettering Cancer Center. Gerstner Sloan Kettering Graduate School of Biomedical Sciences [internet]. U.S. Esophagectomy surgery: a brief overview for family and friends
- Oxford University Hospitals [internet]: NHS Foundation Trust. National Health Service. U.K.; Discharge after an oesophagectomy or an oesophagogastrectomy







